

There have been a lot of accusations of conspiracy theories, fear-mongering and pseudoscience being used against those who have posted contrary information, links, articles and videos through this coronavirus pandemic, and theories of what might be coming in the future.
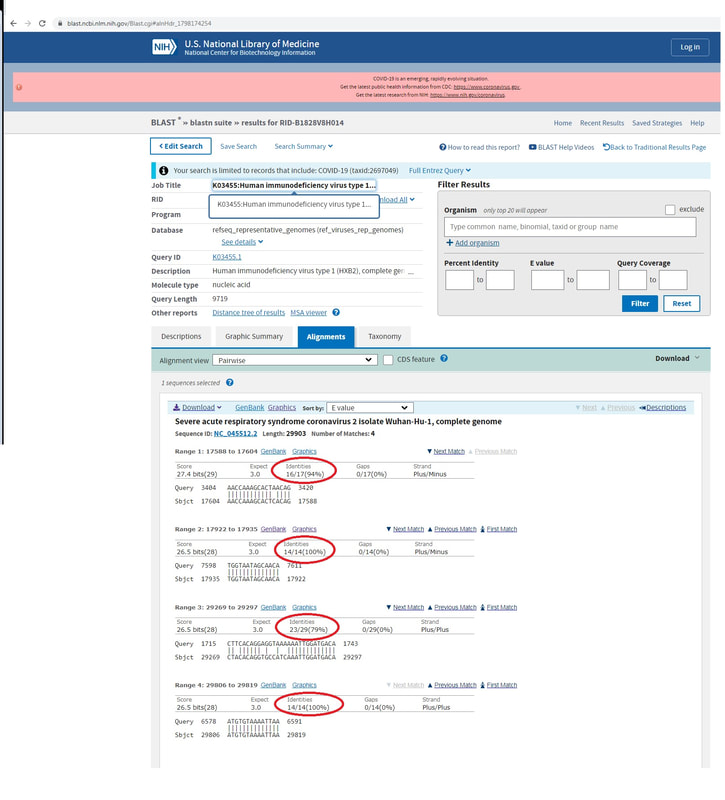
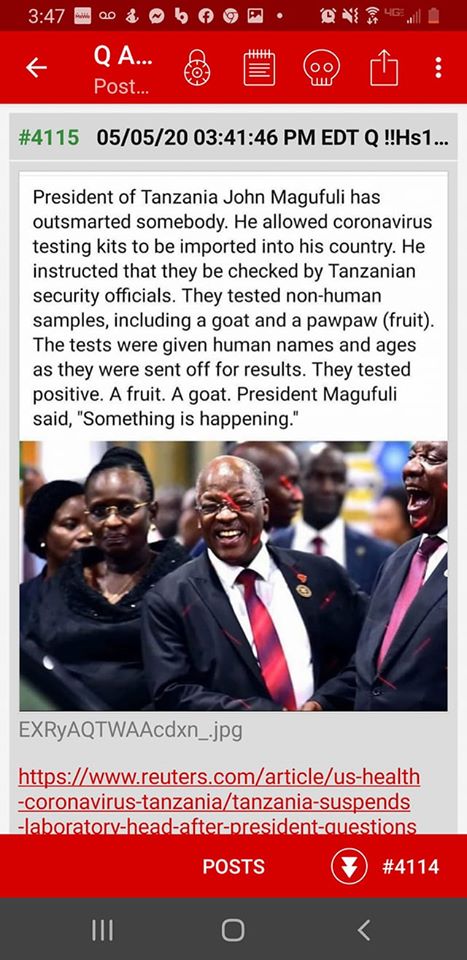
Slowly, more of the alleged theories are appearing to be coming true. More studies are showing the virus was man-made in a lab in Wuhan, China. Studies are showing the PCR testing for coronavirus is inaccurate but being used by the WHO and world governments to make radical changes to restrict our way of life. Classifying COVID-19 deaths is a complete scam, orchestrated by the WHO to cause fear amongst populations, by classifying deaths by any chronic disease, shooting, suicide, or other cause as being from the virus, and the mortality statistics then promoted by a biased and alarmist media.
More accurate statistics of the plandemic are emerging, of a survival rate of 99.9% on average, with very little to no medical treatments available and no coronavirus vaccine. So why all the fuss?
Despite having many less incidences and deaths now, or nearly none at all now, we are seeing tighter restrictions in workplaces, having to give names and contact details prior to entry into shops or cafes, being recommended to wear masks when we go out now (but not earlier in the plandemic when there were more cases!)... what other restrictions do the authorities have in mind?
Well, here's a new one. Are you ready and wanting to travel, access various services or enter your workplace, when restrictions are allegedly "reduced"? Well, make sure you have your "COVI-PASS" digital passport ready to show the authorities, to prove who you are and that you have been a good and faithful citizen with up-to-date coronavirus vaccination, immunity test status to the coronavirus, and a good health rating. This is highly reminiscent of Nazi Germany...
The COVI-PASS is developed and available from a UK cyber security firm (VST Enterprises), and has now been accepted under contract by the United Nations for "various projects", including the post-coronavirus situation. VST say on their website that the digital passport will be expanded to be a much broader personal ID and health passport to cover all personal identification, financial transactions, health testing and history, and proof of vaccinations. Their clients and users of the digital health passport include private companies, airlines, hotel chains and leisure organisations. They say that the COVI-PASS will facilitate safe return to work and life. Why, when cases have dropped almost to nothing, naturally? More details here - https://v-healthpassport.co.uk/
The COVI-PASS is the implementation of the outcomes of the world-wide digital ID plans from the ID2020 summit in 2018. The ID2020 alliance believes it is a human right to "prove one's identity". No, a right to PRIVACY is an essential human right. Bill Gates and Microsoft are an alliance partner to the ID2020 project. More on this alliance can be read here - https://id2020.org/
If you value your right to privacy and right to choose your health options, I guess these services, and maybe more, might be limited to you in the near future. Unless you send a clear message to your governments, employers and companies that you will not be a part of their New World Order of authoritarian control of your health and your life.
Slowly, more of the alleged theories are appearing to be coming true. More studies are showing the virus was man-made in a lab in Wuhan, China. Studies are showing the PCR testing for coronavirus is inaccurate but being used by the WHO and world governments to make radical changes to restrict our way of life. Classifying COVID-19 deaths is a complete scam, orchestrated by the WHO to cause fear amongst populations, by classifying deaths by any chronic disease, shooting, suicide, or other cause as being from the virus, and the mortality statistics then promoted by a biased and alarmist media.
More accurate statistics of the plandemic are emerging, of a survival rate of 99.9% on average, with very little to no medical treatments available and no coronavirus vaccine. So why all the fuss?
Despite having many less incidences and deaths now, or nearly none at all now, we are seeing tighter restrictions in workplaces, having to give names and contact details prior to entry into shops or cafes, being recommended to wear masks when we go out now (but not earlier in the plandemic when there were more cases!)... what other restrictions do the authorities have in mind?
Well, here's a new one. Are you ready and wanting to travel, access various services or enter your workplace, when restrictions are allegedly "reduced"? Well, make sure you have your "COVI-PASS" digital passport ready to show the authorities, to prove who you are and that you have been a good and faithful citizen with up-to-date coronavirus vaccination, immunity test status to the coronavirus, and a good health rating. This is highly reminiscent of Nazi Germany...
The COVI-PASS is developed and available from a UK cyber security firm (VST Enterprises), and has now been accepted under contract by the United Nations for "various projects", including the post-coronavirus situation. VST say on their website that the digital passport will be expanded to be a much broader personal ID and health passport to cover all personal identification, financial transactions, health testing and history, and proof of vaccinations. Their clients and users of the digital health passport include private companies, airlines, hotel chains and leisure organisations. They say that the COVI-PASS will facilitate safe return to work and life. Why, when cases have dropped almost to nothing, naturally? More details here - https://v-healthpassport.co.uk/
The COVI-PASS is the implementation of the outcomes of the world-wide digital ID plans from the ID2020 summit in 2018. The ID2020 alliance believes it is a human right to "prove one's identity". No, a right to PRIVACY is an essential human right. Bill Gates and Microsoft are an alliance partner to the ID2020 project. More on this alliance can be read here - https://id2020.org/
If you value your right to privacy and right to choose your health options, I guess these services, and maybe more, might be limited to you in the near future. Unless you send a clear message to your governments, employers and companies that you will not be a part of their New World Order of authoritarian control of your health and your life.

 RSS Feed
RSS Feed