

One of the most controversial and tragic in all of the events over the past 3 years, despite assurances of the so-called health experts and government officials, is the effects of the "CV-19 carrot" (the so-called "prevention/treatment") on pregnant women and foetuses.
In 2021 I reported on a CDC-funded study which showed an extremely high rate of miscarriages and stillbirths in pregnant women who had the mRNA shots, at approximately 82% (Shimabukuro et al., 2021). But the authors of the study ignored the data and still claimed the carrots were perfectly safe! An independent study reviewed their data some months later and reported issues with their data and explicitly concluded an 82-92% pregnancy loss that was ignored in the original study (Brock & Thornley, 2021). This finding was dismissed by the mRNA carrot manufacturers, and medical professionals, and any posts warning people on this (including mine) were fact-checked as "false" by the social media platforms, and anyone posting such information were censored and thrown in FB jail.
Given a bit more time and the truth always comes out, or becomes harder to hide...
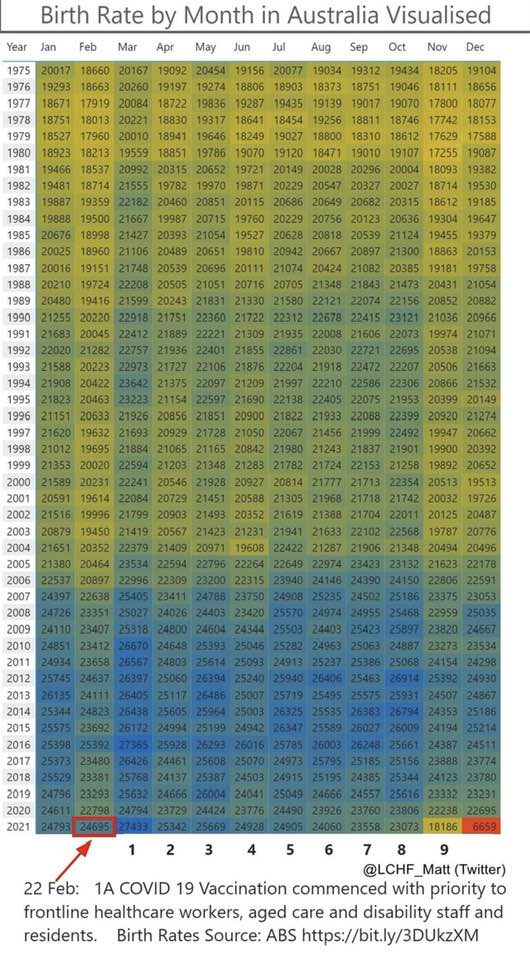
The most current statistics of birth rates from the Australian Bureau of Statistics (ABS), shows the tragic results of the mRNA carrots that were mandated/forced/coerced to pregnant women, despite no safety testing every being done, as pregnant women are not allowed to be used in medical trials.
Australias's birth rates have been steadily increasing from 18,000-20,000 in 1975 to approximately 22,000-25,000 in 2019-2020. Until the mRNA carrots were introduced in February 2021... (ABS, 2022).
Since May 2021, being 3 months from the start of the carrot program, the birth rates have dropped EVERY MONTH from 25,669 to just over 23,000 in October 2021... to just over 18,000 in November 2021, the lowest since well before 1975...
To just 6,659 in December 2021.
That's an approximately 75% DROP in birth rates in 6 months, or in just 10 months since the carrots were introduced, which is coincidentally the same as the duration of a human pregnancy at approximately 40 weeks or 10 months.
The data is not just about the drop in birth rates, but the approximate 20,000 babies who died from the the effects of the mRNA carrots injected during pregnancy.
The 2022 ABS data has not yet been released.
I heard of so many anecdotal stories of mothers losing their babies in pregnancy, from spontaneous abortions and miscarriages in 2021 and 2022. But some people believe that anecdotal evidence bears no scientific merit, but anecdotal evidence is ALWAYS seen first, before published studies. In new situations, anecdotal evidence MUST always be seen as the highest form of scientific evidence.
So it appears that the abovementioned 2 studies on the dangers of the carrots in pregnant women were tragically right. The heads of some companies, health officials, employers and others responsible, need to be held accountable for this, with compensation for the women affected, fines for the companies and directors, and perhaps even jail time for health officials who said the carrots were "safe and effective".
Stay healthy.
References:
Australian Bureau of Statistics (ABS). (2022). Births, by year and month of occurrence, by state. Retrieved 14th November 2022 from https://explore.data.abs.gov.au/vis?tm=births&pg=0&df[ds]=ABS_ABS_TOPICS&df[id]=BIRTHS_MONTH_OCCURRENCE&df[ag]=ABS&df[vs]=1.0.0&hc[Measure]=Births&pd=1975%2C&dq=1..AUS.A&ly[cl]=TIME_PERIOD&ly[rw]=MONTH_OCCUR&fbclid=IwAR1TND3_bpZfe84RWBXD6BNqZfliOUlQzIQUtWUQWT9tbuVD_1chAHOwCGM
Brock, A.R., & Thornley. S. (2021). Spontaneous Abortions and Policies on COVID-19 mRNA Vaccine Use During Pregnancy. Science, Public Health Policy, and the Law, 4. 130–143
Shimabukuro, T.T., Kim, S.Y., Myers, T.R., Moro, P.L., Oduyebo, T., Panagiotakopoulos, L., Marquez, P.L., Olson, C.K., Liu, R., Chang, K.T., Ellington, S.R., Burkel, V.K., Smoots, A.N., Green, C.J., Licata, C., Zhang, B.C., Alimchandani, M., Mba-Jonas, A., Martin, S.W., Gee, K.M., & Meaney-Delman, D.M. (2021). Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons, New England Journal of Medicine, 384 (24), 2273–2282. https://doi.org/10.1056/NEJMoa2104983
In 2021 I reported on a CDC-funded study which showed an extremely high rate of miscarriages and stillbirths in pregnant women who had the mRNA shots, at approximately 82% (Shimabukuro et al., 2021). But the authors of the study ignored the data and still claimed the carrots were perfectly safe! An independent study reviewed their data some months later and reported issues with their data and explicitly concluded an 82-92% pregnancy loss that was ignored in the original study (Brock & Thornley, 2021). This finding was dismissed by the mRNA carrot manufacturers, and medical professionals, and any posts warning people on this (including mine) were fact-checked as "false" by the social media platforms, and anyone posting such information were censored and thrown in FB jail.
Given a bit more time and the truth always comes out, or becomes harder to hide...
The most current statistics of birth rates from the Australian Bureau of Statistics (ABS), shows the tragic results of the mRNA carrots that were mandated/forced/coerced to pregnant women, despite no safety testing every being done, as pregnant women are not allowed to be used in medical trials.
Australias's birth rates have been steadily increasing from 18,000-20,000 in 1975 to approximately 22,000-25,000 in 2019-2020. Until the mRNA carrots were introduced in February 2021... (ABS, 2022).
Since May 2021, being 3 months from the start of the carrot program, the birth rates have dropped EVERY MONTH from 25,669 to just over 23,000 in October 2021... to just over 18,000 in November 2021, the lowest since well before 1975...
To just 6,659 in December 2021.
That's an approximately 75% DROP in birth rates in 6 months, or in just 10 months since the carrots were introduced, which is coincidentally the same as the duration of a human pregnancy at approximately 40 weeks or 10 months.
The data is not just about the drop in birth rates, but the approximate 20,000 babies who died from the the effects of the mRNA carrots injected during pregnancy.
The 2022 ABS data has not yet been released.
I heard of so many anecdotal stories of mothers losing their babies in pregnancy, from spontaneous abortions and miscarriages in 2021 and 2022. But some people believe that anecdotal evidence bears no scientific merit, but anecdotal evidence is ALWAYS seen first, before published studies. In new situations, anecdotal evidence MUST always be seen as the highest form of scientific evidence.
So it appears that the abovementioned 2 studies on the dangers of the carrots in pregnant women were tragically right. The heads of some companies, health officials, employers and others responsible, need to be held accountable for this, with compensation for the women affected, fines for the companies and directors, and perhaps even jail time for health officials who said the carrots were "safe and effective".
Stay healthy.
References:
Australian Bureau of Statistics (ABS). (2022). Births, by year and month of occurrence, by state. Retrieved 14th November 2022 from https://explore.data.abs.gov.au/vis?tm=births&pg=0&df[ds]=ABS_ABS_TOPICS&df[id]=BIRTHS_MONTH_OCCURRENCE&df[ag]=ABS&df[vs]=1.0.0&hc[Measure]=Births&pd=1975%2C&dq=1..AUS.A&ly[cl]=TIME_PERIOD&ly[rw]=MONTH_OCCUR&fbclid=IwAR1TND3_bpZfe84RWBXD6BNqZfliOUlQzIQUtWUQWT9tbuVD_1chAHOwCGM
Brock, A.R., & Thornley. S. (2021). Spontaneous Abortions and Policies on COVID-19 mRNA Vaccine Use During Pregnancy. Science, Public Health Policy, and the Law, 4. 130–143
Shimabukuro, T.T., Kim, S.Y., Myers, T.R., Moro, P.L., Oduyebo, T., Panagiotakopoulos, L., Marquez, P.L., Olson, C.K., Liu, R., Chang, K.T., Ellington, S.R., Burkel, V.K., Smoots, A.N., Green, C.J., Licata, C., Zhang, B.C., Alimchandani, M., Mba-Jonas, A., Martin, S.W., Gee, K.M., & Meaney-Delman, D.M. (2021). Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons, New England Journal of Medicine, 384 (24), 2273–2282. https://doi.org/10.1056/NEJMoa2104983


 RSS Feed
RSS Feed