
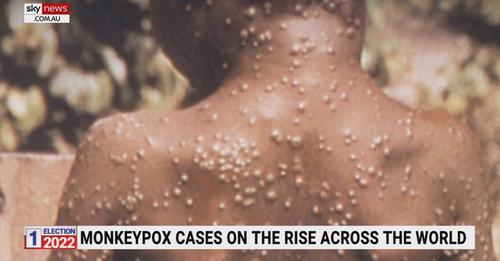
You might have seen recent news stories of another infection suddenly appearing, this time being monkeypox. Geez, we've only had a few weeks of flu propaganda after 2 solid years of coronavirus BS, and now monkeypox wants its share of the headlines!
But judging by the many memes that are circulating on social media already in just a few days, and comments on news and government posts on the topic, no-one is buying into the BS.
I did post about smallpox/monkeypox in 2021 when there were more than a few "coincidences" that ocurred around that time, or in recent times on this topic, including:
1. In an interview in November 2021, Bill Gates warns of a smallpox terror attack, and recommends governments put billions of dollars into funding prevention (Independent, 2021)
2. 1 week after Bill mentioned smallpox in an interview, there were news reports of 15 vials of smallpox found in a freezer in a pharmaceutical company (Merck) freezer and the FBI and CDC were called to investigate (Yahoo News, 2021)
3. Or a group of Canadian scientists in 2017 who RECREATED a horse pox virus, similar to smallpox, which was previously extinct (Centre for Infectious Disease Research and Policy, 2017). Pretty much for laughs... They said "This shouldn't surprise anyone. This is just molecular biology, and we've had the ability to do this for ages"
4. The CDC announced a monkeypox infection found in the US in November 2021
5. US Government buys 1.7 million doses of smallpox vax in 2021. And the Canadian military bought $2.3 million of smallpox doses, and Public Health Canada another $12.8 million
6. In 2015-2017, SIGA Technologies trialled their new TPOXX smallpox vaccine in Africa and USA
7. The FDA approved the new TPOXX vax for smallpox in July 2018! (FDA, 2018)
8. The FDA approved a new and fast-tracked medication for smallpox in July 2021! (FDA, 2021).
Why all this fuss, research and many millions or more in funding, all for an infection which was allegedly announced as eradicated in 1970 by the WHO?! Are they expecting this infection, or a variation of it, to be coming back again, or a new pandemic?
As per the current pandemic, something truly stinks in these new developments in the last few days of moneypox, erm, sorry that was a typo...
Be sceptical, aware, and informed. Be healthy!
References:
Centre for Infectious Disease Research and Policy. (2017). Canadian group creates poxvirus, prompting dual-use discussion. Retrieved 18th November 2021 from www.cidrap.umn.edu/news-perspective/2017/07/canadian-group-creates-poxvirus-prompting-dual-use-discussion
FDA. (2018). FDA approves the first drug with an indication for treatment of smallpox. Retrieved 21st May 2022 from www.fda.gov/news-events/press-announcements/fda-approves-first-drug-indication-treatment-smallpox
FDA. (2021). FDA approves drug to treat smallpox. Retrieved 21st May 2022 from www.fda.gov/drugs/news-events-human-drugs/fda-approves-drug-treat-smallpox
Independent. (2021). Bill Gates warns of smallpox terror attacks as he seeks research funds. Retrieved 18th November 2021 from www.independent.co.uk/news/science/bill-gates-smallpox-terror-attack-b1958789.html
Yahoo News. (2021). FBI investigating vials labeled 'smallpox' found in lab near Philadelphia. Retrieved 18th November 2021 from www.yahoo.com/news/vials-labeled-small-pox-found-in-lab-near-philadelphia-003127682.html
World Health Organisation (WHO). (2021). Smallpox. Retrieved 18th November 2021 from https://www.who.int/health-topics/smallpox#tab=tab_1
But judging by the many memes that are circulating on social media already in just a few days, and comments on news and government posts on the topic, no-one is buying into the BS.
I did post about smallpox/monkeypox in 2021 when there were more than a few "coincidences" that ocurred around that time, or in recent times on this topic, including:
1. In an interview in November 2021, Bill Gates warns of a smallpox terror attack, and recommends governments put billions of dollars into funding prevention (Independent, 2021)
2. 1 week after Bill mentioned smallpox in an interview, there were news reports of 15 vials of smallpox found in a freezer in a pharmaceutical company (Merck) freezer and the FBI and CDC were called to investigate (Yahoo News, 2021)
3. Or a group of Canadian scientists in 2017 who RECREATED a horse pox virus, similar to smallpox, which was previously extinct (Centre for Infectious Disease Research and Policy, 2017). Pretty much for laughs... They said "This shouldn't surprise anyone. This is just molecular biology, and we've had the ability to do this for ages"
4. The CDC announced a monkeypox infection found in the US in November 2021
5. US Government buys 1.7 million doses of smallpox vax in 2021. And the Canadian military bought $2.3 million of smallpox doses, and Public Health Canada another $12.8 million
6. In 2015-2017, SIGA Technologies trialled their new TPOXX smallpox vaccine in Africa and USA
7. The FDA approved the new TPOXX vax for smallpox in July 2018! (FDA, 2018)
8. The FDA approved a new and fast-tracked medication for smallpox in July 2021! (FDA, 2021).
Why all this fuss, research and many millions or more in funding, all for an infection which was allegedly announced as eradicated in 1970 by the WHO?! Are they expecting this infection, or a variation of it, to be coming back again, or a new pandemic?
As per the current pandemic, something truly stinks in these new developments in the last few days of moneypox, erm, sorry that was a typo...
Be sceptical, aware, and informed. Be healthy!
References:
Centre for Infectious Disease Research and Policy. (2017). Canadian group creates poxvirus, prompting dual-use discussion. Retrieved 18th November 2021 from www.cidrap.umn.edu/news-perspective/2017/07/canadian-group-creates-poxvirus-prompting-dual-use-discussion
FDA. (2018). FDA approves the first drug with an indication for treatment of smallpox. Retrieved 21st May 2022 from www.fda.gov/news-events/press-announcements/fda-approves-first-drug-indication-treatment-smallpox
FDA. (2021). FDA approves drug to treat smallpox. Retrieved 21st May 2022 from www.fda.gov/drugs/news-events-human-drugs/fda-approves-drug-treat-smallpox
Independent. (2021). Bill Gates warns of smallpox terror attacks as he seeks research funds. Retrieved 18th November 2021 from www.independent.co.uk/news/science/bill-gates-smallpox-terror-attack-b1958789.html
Yahoo News. (2021). FBI investigating vials labeled 'smallpox' found in lab near Philadelphia. Retrieved 18th November 2021 from www.yahoo.com/news/vials-labeled-small-pox-found-in-lab-near-philadelphia-003127682.html
World Health Organisation (WHO). (2021). Smallpox. Retrieved 18th November 2021 from https://www.who.int/health-topics/smallpox#tab=tab_1


 RSS Feed
RSS Feed