
What is measles? In this current (alleged) time of "outbreaks" of measles, I will explain the symptoms, and answer many questions about how dangerous is measles, including why are might be seeing more of it, how you can prevent this infection, and how it can be treated.
If you think the measles alerts in Australia are a bit much, the USA has gone to extremes with several cities mandating compulsory MMR vaccinations where there might be just 1-5 active measles cases in an entire city, or face fines or jail. Another city council tried to force all non-vaccinated people to stay at home for a month until the outbreak is over. Legal action was taken against the council, and the curfew was lifted when a judge found the action to be unlawful. As you will see in the details below, the real causes of measles outbreaks are perhaps not what you think, nor caused by those who are not up to date with their shots... read on!
This article started out to be a brief one to counter the government and medical propaganda about measles and to alleviate the fear and misinformation that measles is a dangerous health concern. This article is comprehensive and detailed, and answers many questions about measles. This article is fully referenced from published research, with all references and links included.
What is measles?
Measles is a highly contagious viral infection (not a disease!) which is also known as rubeola and is very common in childhood. It can take 10 to 14 days after being exposed to develop measles, although simply being exposed to the virus doesn't mean that you will catch the infection! (Mayo Clinic, 2019).
Measles is transmitted via the respiratory tract, in droplets from an infected person which can remain in the air for up to 2 hours (Orenstein, Perry & Halsey, 2004; Paules, Marston & Fauci, 2019).
Measles is traditionally an infection of children under 5 years of age and those with poor nutritional status, especially a vitamin A deficiency (Paules, Marston & Fauci, 2019). Wouldn't it make more sense to fix the cause of poor nutrition, as a safer form of prevention?!
What are the symptoms of measles?
Measles symptoms include, usually in this order (Mayo Clinic, 2019):
- fever
- dry cough
-runny nose
- sore throat
- inflamed eyes (conjunctivitis)
- tiny white spots with blue-white centres on a red background found inside the mouth, lining the cheek (Koplik's spots)
- a skin rash, with large flat blotches that flow into one another.
How long does measles last?
Measles starts with a fever, and worsening symptoms as above for 2-4 days before the skin rash appears (and the fever subsides) and the number of lesions increase for 2-3 days. The rash lasts for 3-7 days before fading. The cough which accompanies measles can last for about 10 days (Orenstein, Perry & Halsey, 2004).
Most people recover uneventfully after 1 week of illness (Paules, Marston, & Fauci, 2019).
How does measles spread?
Measles is spread via mucus droplets through the air, through coughing or sneezing, or touching surfaces and poor hygiene. There is a communicable period of about 8 days when someone with measles can spread the virus to others, usually about 4 days before the rash appears, and for about 4 days after the rash appears (Mayo Clinic, 2019).
Numerous outbreaks of measles can occur even in highly vaccinated populations, especially in children who attend group social events, as the period of highest transmission to others occurs in the first few days of illness before the rash appears (Orenstein, Perry & Halsey, 2004).
Interestingly, but not well known or talked about, is that the MMR vaccine (allegedly to prevent transmission and provide immunity to measles) is a LIVE virus vaccine, meaning that the measles virus, mumps virus, and rubella (German measles) virus in the vaccine are all ALIVE, albeit weakened. Weakened means that it can still cause the infection to which it is allegedly protecting you from!
What are the measles vaccines?
There are several measles vaccines available in Australia, as a combination of several vaccine antigens in one shot:
- MMR-II (Seqirus, 2006) - the most common trivalent measles vaccine, for children over 12 months of age and adults. The same dose is used for babies, children and adults. A follow-up dose is required, but no details are given by the manufacturer for this.
- Priorix (GSK, 2019) - a trivalent vaccine, containing 3 live viruses - measles, mumps and rubella, and given to children over 12 months of age, or adults. A second dose in children is required at 4-6 years of age.
- Priorix Tetra (GSK, 2019) - a quadrivalent vaccine, containing 4 live viruses - measles, mumps, rubella and varicella (chicken pox), for use in children over 12 months of age, or adults, with the same dose being given for each age group. No details given for subsequent doses
- ProQuad (Sequiris, 2018) - a quadrivalent vaccine, containing 4 live viruses - measles, mumps, rubella and varicella (chicken pox), for use in children over 12 months of age, or adults. The time and number of doses will be "determined by your doctor". Also to note for this vaccine (as per the manufacturer's consumer information) is "At least one month should elapse between a dose of ProQuad and all other vaccines". But then this follows in the next sentence: "Your doctor will decide if ProQuad should be given with other vaccines" . What?!
What are some ingredients in the measles vaccines?
The MMR-II vaccine contains chicken embryo cells, human albumin, cow foetus serum, sorbitol, sucrose, pig gelatin, neomycin (an antibiotic) (Australian Government Department of Health, 2018a).
The Priorix vaccine contains lactose, neomycin, sorbitol and mannitol (sugar alcohols) (Australian Government Department of Health, 2018b).
Very recently, an independent Italian research group called Corvelva, has been performing detailed research into the ingredients of the major scheduled vaccines, and finding unbelievable things added to the vaccines or contaminated in the vaccines. Their most recent investigation (April 2019) and resulting disclosure of findings was on the Priorix Tetra (GSK, 2019; Corvelva 2019a) MMRV (Measles, Mumps, Rubella and Varicella or chicken pox) vaccine. In summary, Corvelva found:
- Very low to negligible amounts of rubella (German measles) virus, far lower than it should have, to the point of being "not detected" in the vaccine, hence the scientists questioning its effectiveness in creating immunity
- Contamination with many live organisms, of which many are dangerous (Corvelva, 2019a):
- Proteobacteria
- Nematodes - parasitic roundworms
- Influenza A - which can cause flu infections
- Enterovirus - a group of viruses which can cause many infectious conditions
- Hepatitis C virus - very dengerous virus capable of causing liver disease
- Hepatitis B virus - another very dangerous virus which causes liver disease
- Coronavirus - which can cause respiratory infections
- Rous sarcoma virus - which causes bone cancer
- Many animal viruses - from pigs, birds, monkeys, horses
- And HIV. Yes, The MMRV vaccine contains HIV, the virus associated with AIDS.
Is measles dangerous or deadly?
The World Health Organisation claim that measles kills 100,000 people per year (Mayo Clinic, 2019), but almost all of these are in developing countries (with poor nutrition, sanitation and hygiene). Mortality rates from measles in developing countries is 10-100 times greater than in developed countries (Orenstein, Perry & Halsey, 2004).
While measles is generally a benign or mild condition in about 99% of those infected, measles can cause complications in many body systems or organs. Pneumonia is the most severe complication of measles, usually as a result of a secondary infection of the respiratory tract, but diarrhoea and malnutrition during the illness can also contribute to mortality (Orenstein, Perry & Halsey, 2004).
Being malnourished, which is common in undeveloped countries, is the main reason for measles mortality, with malnourished children having a mortality rate 200-400 times greater than measles-affected children in developed countries with poor sanitation and inadequate medical care (Gabr, 1987, pp1–21; Hoeprich, 1977, pp691-696). However in well-nourished children, measles is NOT a serious infection (Hoeprich, 1977, pp691-696).
Some published studies show that measles can be more deadly when children are exposed to the virus within a family home, with this likely being caused from a prolonged exposure to the virus, rather than from a casual exposure to an infectious person outside the home (Orenstein, Perry & Halsey, 2004).
Measles can cause a more serious infection or complications in someone who immunocompromised (such as with cancer, organ transplants, HIV or other existing infections or conditions) (Paules, Marston & Fauci, 2019), or if someone is taking immunosuppressive medications (such as NSAIDs, steroids, chemotherapy, or other medications), or is malnourished (especially a vitamin A or protein deficiency) (Orenstein, Perry & Halsey, 2004; British Medical Journal, 1976).
Back before the MMR vaccine was introduced (in 1963 in some countries, and later in others), parents used to hold a "measles party"! If a child were to contract measles, the parents would invite other parents with young children to their house so the kids could play together and be exposed to the measles virus. Doing so may or may not result in other children getting measles, but most children then DID get measles naturally (at much higher rates than now) but the children exposed to measles would develop a LIFELONG immunity and protection to measles.
Can I contract measles from the MMR vaccine?
Yes.
Health departments acknowledge that "vaccine-derived" measles CAN and DOES occur approximately 5-12 days after measles/MMR vaccination (Australian Government Department of Health, 2019a).
The government health authorities claim that the vaccine-derived form of measles is not transmissible and should not be classified as measles, but many published studies contradict this belief (Australian Government Department of Health, 2019a; Rosen et al., 2014).
Interestingly the government website (Australian Government Department of Health, 2019a) contradicts themselves on this issue, stating that if someone had the MMR vaccine in a period of 3 weeks before contracting measles, that serology testing should be done to determine whether the person has the wild or natural type, or the vaccine strain virus infection, and if the wild type was not detected, that the diagnosis IS measles. But they then state that serology testing of a suspected measles case is useless for diagnosis if they received the MMR vaccine 8 days to 8 weeks before testing. Huh?!
Can I contract measles from an unvaccinated person?
Only if they have measles, and only they are in the infectious period of the infection. The likelihood of this happening is very, very small!
An unvaccinated child or adult who has no symptoms does not have the measles (or any other) virus! So despite the popular hysteria about unvaccinated people, they cannot spread infections they do not have to anyone else! As such, isolating unvaccinated people (who don't have measles) during outbreaks will do nothing to reduce the transmission or incidences of measles.
As shown in this article, research shows that vaccinated people can spread measles to others for a period of 4-6 weeks after vaccination, and they can also contract measles from the MMR vaccination they have just had (Nestibo, Lee, Fonseca, Beirnes, Johnson & Sikora, 2012). Hence children and adults are far more likely to get measles from vaccinated people!
How long does measles immunity last?
If you have had measles (or mumps, or rubella, or any other infection) your immune system develops antibodies which provides a lifetime of protection against that particular infection!
Sadly, the same doesn't occur when one has a simulated infection in the form of a vaccine. Because with a vaccine you are bypassing the normal route of entry into the body (via the respiratory and/or digestive tracts, where your innate immune system is present in abundance), so your immune system doesn't work in the same way as a real infection to develop a lifelong immunity from any vaccine.
The short-term duration of "immunity" of a vaccine varies between individuals, with many not developing immunity at all anyway. This short-term immunity creates several larger problems:
- There can be higher rates of measles even when an ever-increasing percentage of the population have been vaccinated, as those vaccinated become no longer immune over time and thus susceptible to measles again
- Higher risk groups, such as pregnant women and their unborn foetuses, are more susceptible to measles and its complications (including foetal deaths) from a waning measles immunity and from increased incidences.
What are the typical medical treatments for measles?
Typical medical treatments for measles include:
1) Fever reducers - using anti-inflammatory or NSAID (non-steroidal anti-inflammatory drugs) such as Ibuprofen (Nurofen etc), Paracetamol or acetaminophen drugs. These drugs can reduce some of the SYMPTOMS of the infection, but what they are really doing is stopping the immune system response against the infection, and makes the infection worse. Fevers are a natural immune system response to an infection - the increased body temperature slows down or stops the replication of the pathogens such as the measles virus and even kills them, and also stimulates the production of more infection-fighting white blood cells! Hence why fevers should be supported rather than suppressed (Roesch et al., 2012; Plaza, Hulak, Zhumadilov & Akilzhanova, 2016).
2) Antibiotics - these are either utterly useless against measles, as measles is a VIRAL infection, and antibiotics only kill bacteria... or these can be very damaging and cause a more serious infection, as antibiotics kill good or beneficial bacteria in your digestive tract that actually make your immune system proteins called immunoglobulins! So why kill your immune system, at the time when you NEED it working to fight an infection?
3) Vitamin A - children (and others) with low levels of vitamin A are more at risk of developing measles, and having more serious symptoms. Vitamin A helps as an antioxidant, fights cell damage, and helps to heal the skin, which is a better treatment for measles! (Mayo Clinic, 2019)
What are some natural treatments for measles?
Anything which supports your immune system to do its job to find and fight infections will help against measles, including:
- Vitamin A - as a deficiency of this vitamin can increase the risk of contracting measles, it is also recommended in a measles treatment. Can reduce incidences of measles complications, and reduces mortality by 70-80% in those who developed pneumonia (a complication of measles) (Fawzi, Chalmers, Herrera & Mosteller, 1993; Shetty, 2010, p82).
- Vitamin D - offers immune defence against many pathogens including viruses, by stimulating the body's innate imune system against infections which it hasn't encountered before
- Vitamin C - vitamin C is also seen to be deficient in those with measles (Cemek, Dede, Bayıroğlu, Çaksen, Cemek & Mert, 2006), hence higher doses of vitamin C can support the immune system to fight infections, and reducing the damage from measles virus
- -zinc - essential for good immune system function and skin healing
- Probiotics - improves immune system responses against infections
- Quality multi-vitamin and/or multi-mineral supplements, to reduce deficiencies which weaken the immune system
- Herbal medicines - to improve immune system function and those with antiviral actions
- Breastfeeding - this is extremely important, as breast milk transfers much of the mother's antibodies and immune protection to the baby. If a child hasn't been breastfed, measles can be much more severe (Orenstein, Perry & Halsey, 2004).
- Protein - mortality rates from measles can be reduced by 66% simply with an improved dietary intake, and addressing any nutrient deficiencies or excesses which can affect the function of the immune system, especially of sufficient protein. A lack of protein in the diet, particularly in undeveloped countries, is a major factor in higher measles mortality rates (British Medical Journal, 1976).
Yes!
Remember that you, and your children, have an immune system! Our immune systems have kept the human species alive and healthy for millions of years, despite being exposed to the measles virus, and many thousands of other infectious bacteria, viruses, fungi, and parasites!
So they key to preventing measles (or any other infection) is to keep your immune system strong to do its job. This can be done by looking after your body and your health, by:
- eating a wide variety of quality foods for nutrients your immune system needs
- sleeping well, with good quantity and quality sleep
- reducing stress exposure, and having good stress management or relaxation time
- reducing exposure to toxins and chemicals in your foods and environment
- having a good lifestyle - no smoking, limited or no consumption of alcohol and drugs etc, and some exercise
- having good hygiene practices
- and controversially, limiting physical contact with children or others who have had the MMR vaccine, because as mentioned above, MMR is a LIVE virus vaccine, and studies have shown that those vaccinated with these 3 viruses CAN and DO shed these viruses in their body fluids for a about 4-6 weeks after the vaccine (Nestibo, Lee, Fonseca, Beirnes, Johnson & Sikora, 2012).
Should you (or your child) get the measles/MMR vaccine if you suspect you have (or your child has) measles or any other infection?
Absolutely not.
No vaccines are recommended to be taken when you or a child is already ill, or if immunocompromised, or has a fever. If a child is ill, then they are immunocompromised, and this is a contraindication (a medical factor which is a reason to withhold a medical treatment) as it could cause harm to the person. Immunocompromised people who are vaccinated have a higher risk of complications from the vaccination, including dangerous and severe meningoencephalitis, or a combination of meningitis and encephalitis, being an infection or inflammation of the meninges (protective tissues around the brain and spinal cord) and brain (Paules, Marston & Fauci, 2019).
People who are immunocompromised or on immunosuppressive medications cannot be safely vaccinated with any live virus vaccine (Paules, Marston & Fauci, 2019).
How effective is the measles/MMR vaccine against measles incidences and mortality?
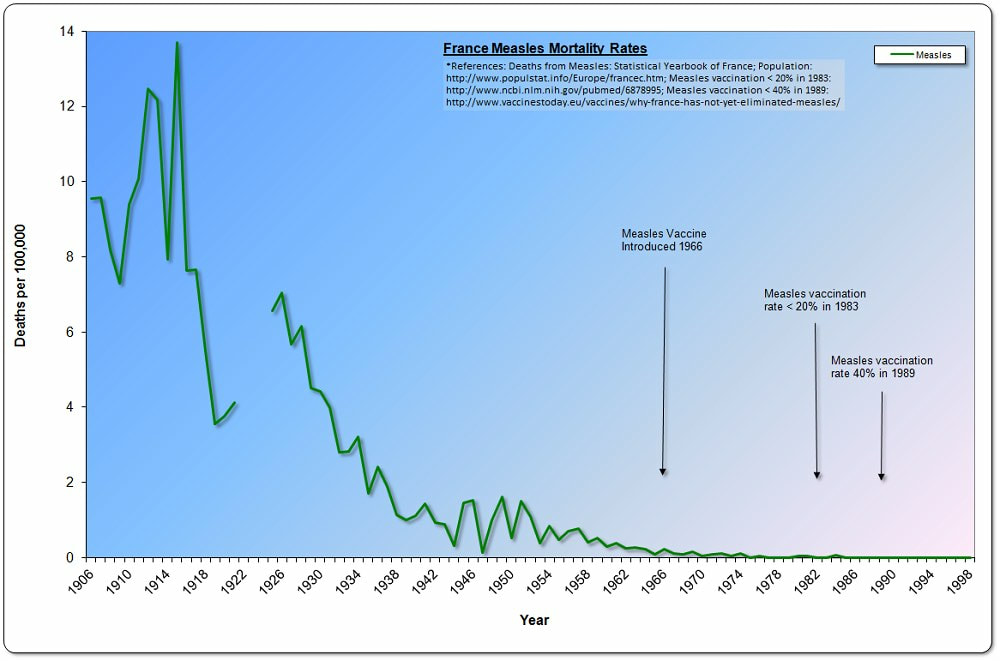
The first measles vaccine was only made available as MMR in 1963 in some countries. By that time the incidences and mortality of measles had already dropped by 99% from their peaks! Rates continued to drop even with only 20-40% of the population vaccinated.
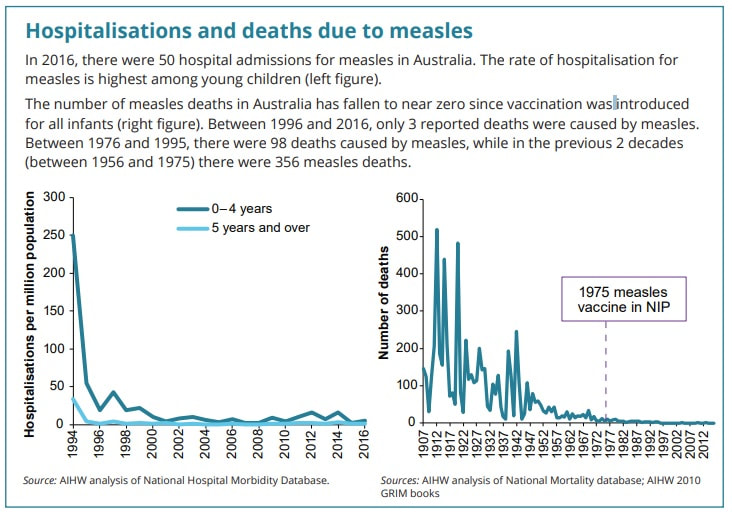
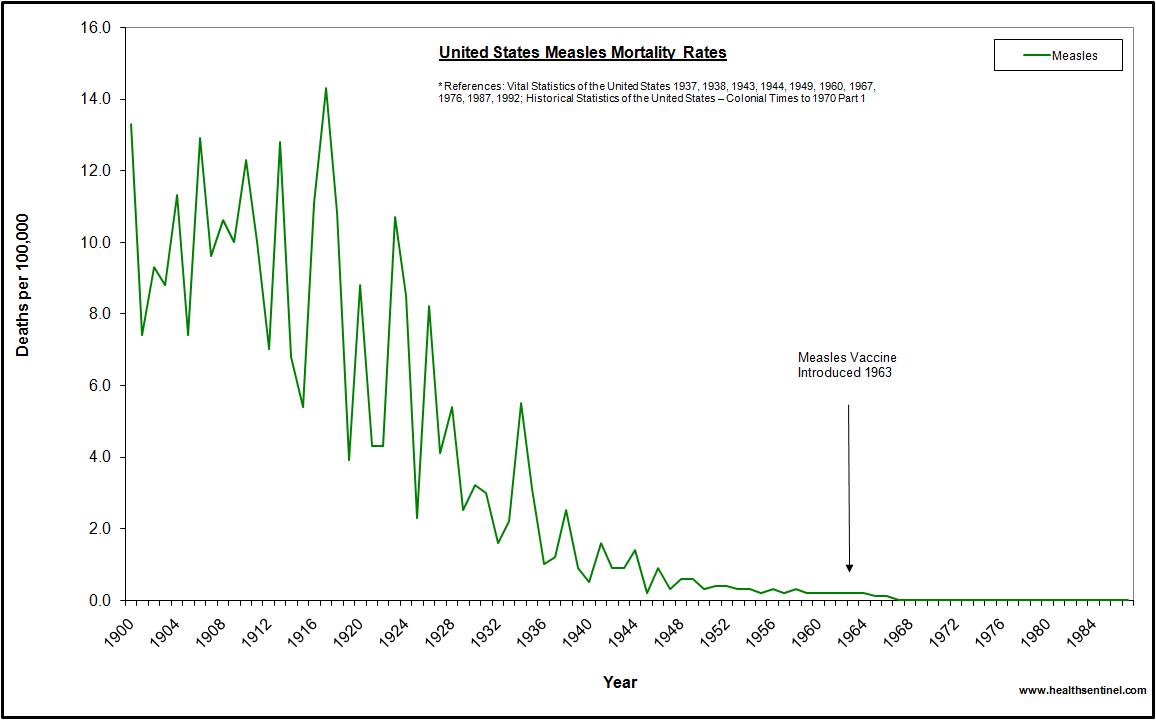
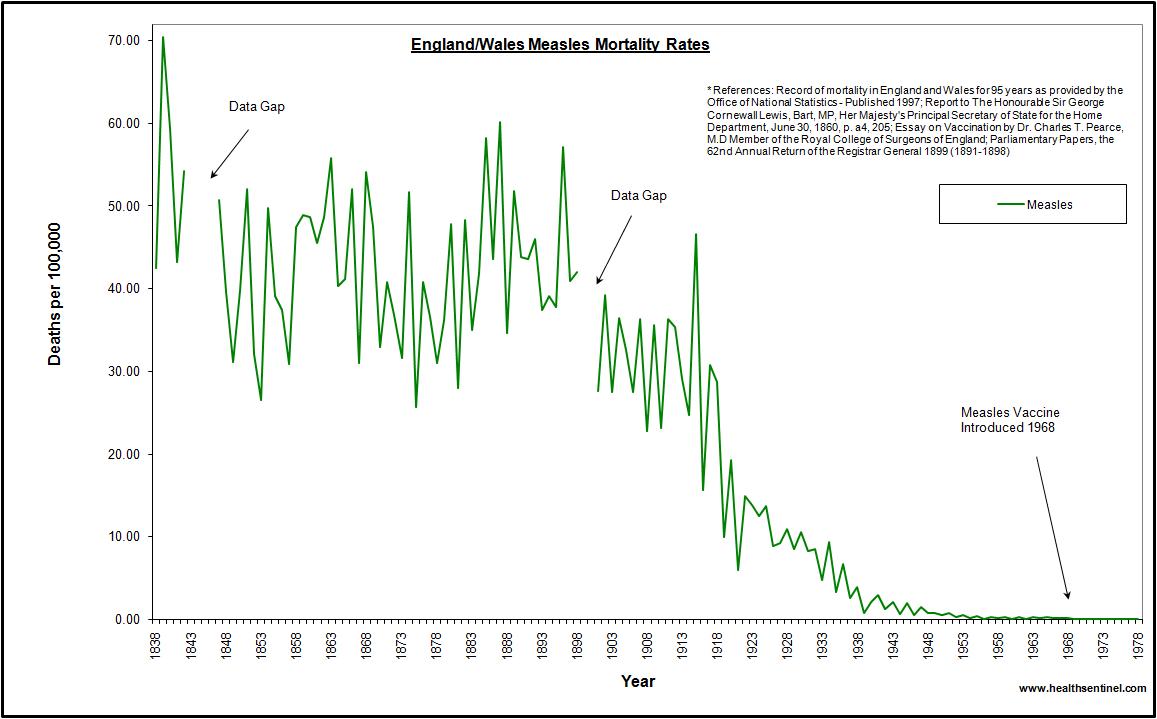
See the attached images for some official referenced statistical charts from various countries showing a huge drop in measles incidences and deaths well before the vaccine was made available.
Figure 1 - Measles hospitalisations and deaths in Australia (Australian Institute of Health and Welfare, 2018).
Figure 2 - Measles mortality in the USA. Reference details in the chart.
Figure 3 - Measles mortality in England and Wales. Reference details in the chart.
Figure 4 - Measles mortality in France. Reference details in the chart.
Despite the results in these charts coming different official sources, they show the same information - a 99% decrease in measles incidences or deaths before the vaccine was introduced.
What these charts do not show are:
1.whether the measles incidences since the vaccine was introduced, are from the wild type measles infection or the vaccine strain
2. the adverse reactions and deaths from the vaccine itself.
To answer the first point, a study published in 2017 investigated a large measles outbreak amongst people who had been recently vaccinated against measles in California in 2015. Using genetic sequencing of samples from the vaccinees with measles symptoms, the study reported that 38% of them were caused by the vaccine strain virus (Roy et al., 2017). Interestingly, in the same study, they mention that the World Health Organisation recommends that the measles virus contain the "type A" measles virus, but that the "wild type A" measles virus no longer exists! So we are being vaccinated with "type A" measles virus to allegedly protect us from the "type A" measles virus in the wild that no longer exists?! How does this make any sense?!
Viruses mutate and adapt to a changing environment. We are told to get flu vaccines annually as they contain different strains of flu virus each year, allegedly to protect us from only those strains. So why are we being vaccinated with a measles strain that no longer exists in the wild?! How will that protect us?
Is getting the MMR vaccine safer than getting measles?
No, not in my opinion, nor when looking at the statistics.
The government and health authorities will tell you that measles in Australia is deadly, and that you should have the MMR vaccine to prevent the disease and complications and possible death. But the last officially recorded death from measles in Australia was in 1995, despite many outbreaks including an outbreak of 168 cases in Sydney in 2012 (National Centre for Immunisation Research and Surveillance, 2016).
In the same period (1995 to 2019) there were 8 deaths attributed to the measles vaccines in Australia, together with 6796 official adverse reaction reports logged. Considering that reporting vaccine adverse events is voluntary and well known to be under-reported to perhaps only 1% of the actual rates, the possible number of vaccine-caused deaths or adverse events would be even more shocking. Even without taking the under-reporting of adverse events into account, the number of deaths which have been officially caused by the measles/MMR vaccines in the past 25 years in Australia are far in excess of the deaths by measles (Therapeutic Goods Administration, 2019).
Would the family members or friends of those who died from the measles/MMR vaccine say that the vaccine was worth a life? I don't believe so. The cost, in terms of lives lost from the vaccine itself, simply do not justify the very low risk of measles in Australia, which can be prevented and treated in other safer and natural ways, if only the public were actually told the truth about measles and the MMR vaccine.
What testing has been done on the MMR vaccine?
Good quality scientific testing for any medical and vaccine products is essential and at a minimum requires a randomised placebo controlled trial. In this scientific protocol, the scientists randomly assign test subjects into 2 groups - one group gets the medication or vaccine, and the other gets an inert placebo substance, and the test subjects don't know which one they are getting.
The purpose of such tests is to check for the action of the medication or vaccine using various physical, biochemical and physiological tests, to confirm the safety and efficacy (the ability to produce the desired result) of the product. An inert placebo, such as a sugar pill or saline (salt water) is usually used, to look at the differences in results between those who are having the substance compared with those who do not have the substance. In effect, the study is looking for the differences in immune response and any side effects between the 2 groups.
The problem is that vaccines are not classified as medications and do not need to undergo the same trials for regulatory approval to be given to the public! So vaccine manufacturers do not perform placebo controlled trials. Instead they compare their vaccine in test subjects to another group who get a different or earlier vaccine. As such, there are NO randomised placebo-controlled trials of any vaccine which truly shows how safe or effective they are.
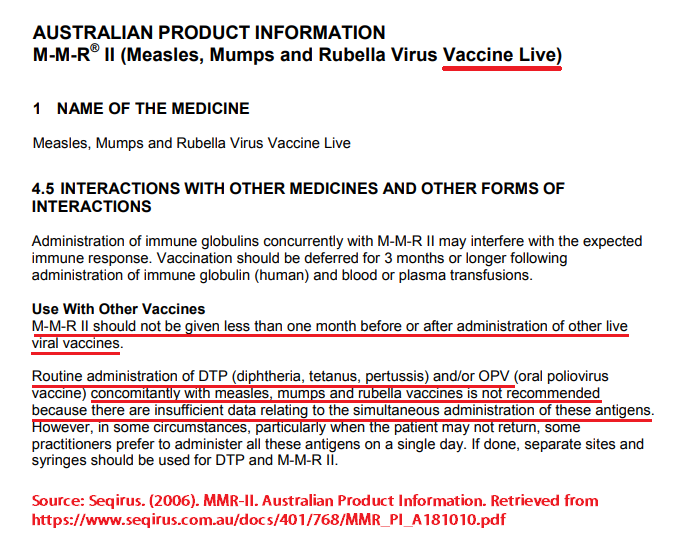
In addition, there are no studies done at all on combined multiple vaccine shots being given to babies, children or adults. NONE! Yet every government vaccination program recommends this practice. But, as seen in this article, some MMR manufacturers even state on their own product information inserts that the vaccine has not been tested for safety together with other vaccines, and some MMR manufacturers recommending that other vaccines NOT be given with MMR by a number of MONTHS.
In 1998 there was a major peer-reviewed study published in the prestigious The Lancet medical journal, authored by Gastrointestinal specialist Doctor Andrew Wakefield, and 10 others. He wasn't the first to point out in a study that autistic children had a high rate of gastrointestinal conditions, but his study became the most widely published and well known. He and his fellow scientists found very similar test results in the gastrointestinal tracts of all children with gut and behavioural issues, 75% had regressed (went backwards in their development, speech and behaviour) after the MMR vaccine and had been diagnosed with autism, and together with previous studies finding the same, that the gut issues appeared to play a part in the behavioural changes in some children (Wakefield et al., 1998).
Wakefield commented in the study that previous studies had found that measles and rubella were already linked to autism disorders, as was the MMR vaccine in other studies, which showed autistic symptoms appearing within a week of the MMR vaccination (Wakefield et al., 1998).
While Wakefield's study was retracted and he was struck off by the medical authorities after the study was published as it caused a huge controversy in the world's media, health authorities and pharmaceutical companies, he NEVER actually said that MMR caused autism in his study - that was a media misinterpretation of the study. What he DID say on this was "we did not prove an association between measles, mumps, and rubella vaccine and the syndrome described" (ie autism), and he concluded with "In most cases, onset of symptoms was after measles, mumps, and rubella immunisation. Further investigations are needed to examine this syndrome and its possible relation to this vaccine" (Wakefield et al., 1998).
So if Dr Wakefield said that he did not find MMR caused autism, does that prove MMR doesn't cause autism? NO! Why, because as he pointed out in his study, PREVIOUS studies had already found that MMR caused gastrointestinal and neurological symptoms, and those studies reported that MMR appeared to be the linked to autism. Since Wakefield's study, over 157 other peer-reviewed and published studies have confirmed his findings, and linked the MMR vaccine to causing autism. This list keeps on growing... and none of these doctors or scientists have been vilified in the media as Dr Wakefield was. The link to all these studies is here:
ttps://www.scribd.com/doc/220807175/157-Research-Papers-Supporting-the-Vaccine-Autism-Link
Should I get the measles/MMR vaccine when I am pregnant?
Absolutely not.
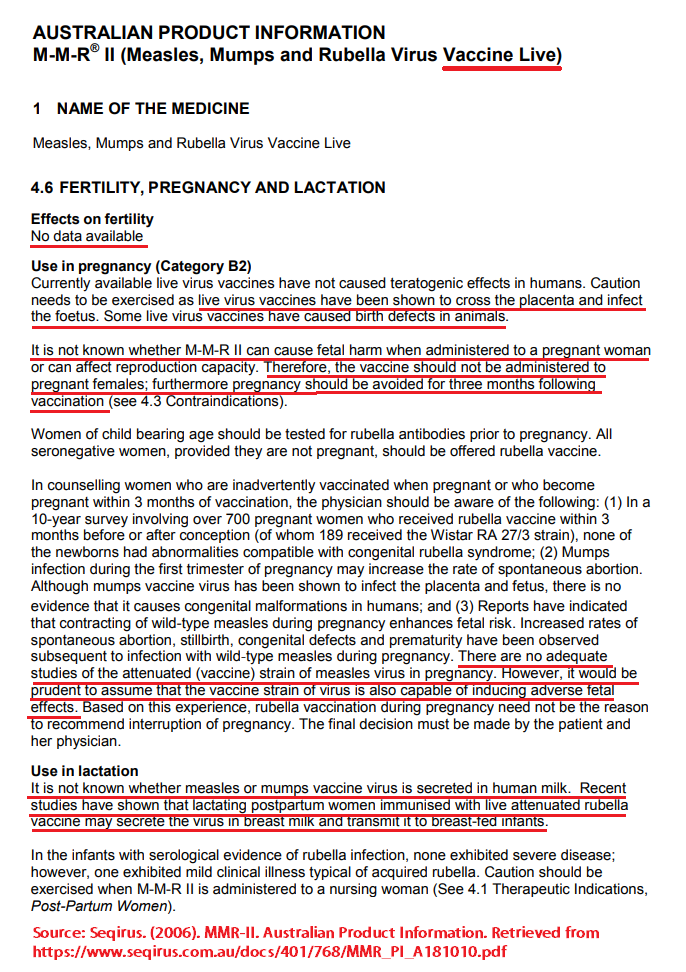
The most common MMR vaccine approved for use in Australia is actually the MMR-II (Seqirus, 2006). The manufacturer's own product information insert (available here: https://www.seqirus.com.au/docs/401/768/MMR_PI_A181010.pdf) has the following statements related to pregnancy:
- "Do not give MMR-II to pregnant females"
- "the possible effects of the vaccine on foetal development are unknown"
- "the vaccine should not be administered to pregnant females"
- "there are no adequate studies of the attenuated (vaccine) strain of measles virus in pregnancy"
- "the vaccine strain of virus is also capable of inducing adverse fetal effects"
- "Women of childbearing age should be advised not to become pregnant for three months after vaccination against rubella (in MMR)".
Figure 5 - MMR-II Product Information statements regarding vaccination in pregnancy (Seqirus, 2006)
So why do doctors and health departments push this on pregnant women? Doctors are supposed to provide "informed consent", to let you know of possible risks beforehand, and for you to decide whether to get it or not, based on being given unbiased information. They are lying if they say it's safe, when this has never actually been proven (see the above or attached screenshot of the MMR vaccine manufacturer's product information ).
The other measles vaccines have very similar statements about avoiding getting these vaccines in pregnancy, as there are NO studies done by the manufacturers for the safety or efficacy of this (or any other) vaccine in pregnancy.
The ProQuad vaccine has similar statements about pregnancy, but "pregnancy should be avoided for 3 months following vaccination" (Seqirus, 2018).
The vaccine manufacturers also suggest avoiding vaccinations when breastfeeding, as the vaccine either has not been tested in lactation, or in the case of MMR-II, that one or more of the live viruses can be secreted in breast milk to transmit the infection to the baby (Seqirus, 2006).
Will herd immunity (95% vaccination rate) or 100% coverage of measles vaccine (as in MMR) prevent or wipe out measles?
No!
In fact we are seeing the opposite - more incidences of measles as more people get the vaccine! It simply is not possible to eliminate every last virus on the planet, so there will always be incidences.
The official government statistics show that 95% of all Australians have been vaccinated (or 93.5% with MMR), with 95% being the alleged theoretical goal for "herd immunity" that is supposed to protect everyone from preventable diseases (Australian Department of Health, 2019b). Studies say that a "near-prefect" immunisation rate of 93-95% is needed to effectively protect against a measles resurgence (Paules, Marston & Fauci, 2019). But clearly this isn't working when Australia and the USA in particular have reached this "herd immunity" level yet we are seeing some of the highest incidences of measles infections in recent times! Clearly, the vaccination program isn't working to protect people, or the "herd immunity" theory is bust. Herd immunity is a theory, and one that has never been proven to work.
The Australian Government prematurely or optimistically declared that the country was "measles-free" in 2014 (Sydney Morning Herald, 2017)! But we are seeing more and more incidences in the past few years, ironically as MORE people are vaccinated. The outbreaks were ALL blamed on travellers visiting countries which had higher rates of measles infections. Shouldn't the vaccine have prevented them getting the infection or spreading it to others?
What may be a major factor for causing the increased incidences despite reaching the "herd immunity" vaccination rate, is the short-term "immunity" that the vaccine offers, as opposed to the lifetime immunity that the natural measles infection offers. Hence it is the failing MMR vaccines causing the measles outbreaks and complications, and not the failure to vaccinate!
What should I do if I still want to get the measles/MMR vaccine?
If, after doing your due diligence and research of the MMR product information inserts from the TGA or the vaccine manufacturers (see the links in the References) and reading published research on MMR (some provided above and in the References), you still want to get the MMR vaccine, that's your choice. However, there are some other steps you can take to minimise the risks of potential side effects and health damage from the vaccine by also looking at:
1) Getting all children tested with the MTHFR genetic test PRIOR to any vaccines - this simple saliva or blood pathology test is available from your GP or Naturopath, and can let you know if your child has a reduced ability to detoxify chemicals (such as vaccine ingredients) or an increased risk of nutrient deficiencies, which are a huge factor in vaccine damage or side effects. MTHFR is another large topic on its own, and I have written several articles on this in the past - see my website or Facebook page
2) Avoid using fever-reducing medications and/or NSAIDs to hide a fever after a vaccine - fevers are generally safe, and are a natural immune system response to a spreading infection, as a way to stop the spreading or kill the infection by increasing the body temperature. Fevers are a natural defence mechanism against infections! (Plaza, Hulak, Zhumadilov & Akilzhanova, 2016). Stopping the fever will make the infection more severe and last longer. Fever-reducing and NSAID medications deplete glutathione, your body's most potent antioxidant which can lead to vaccine damage and side effects. This can be mitigated by seeing a Nutritionist or Naturopath and preparing before any vaccinations. Always monitor temperatures in small children, and keep up fluid and electrolyte intakes
3) Delay and spread out the vaccines - many children simply cannot take all the scheduled vaccines all at the same time, hence why many see health impacts of this, including deaths. This is because there has never been any studies done to show that having multiple vaccines at once are either safe or effective, despite the government health departments and their recommendations to combine vaccines. To reduce issues, the longer you delay the first and subsequent vaccines , the better, and spreading them out so their bodies can deal with the vaccines and recover fully, before getting more. For more information on this, look for information from US-based Paediatrician Dr Paul Thomas in particular, who has performed research on thousands of his own clients to show that autism rates with children on the government schedule is 1:35 (one in 35, the official government statistic), versus 1:438 for those on Dr Thomas's delayed schedule "vaccine-friendly" plan, or just 1:715 in unvaccinated (Thomas, 2019)
4) Never get your children vaccinated when they are ill - the vaccine will place an additional burden on their bodies and make it harder to deal with the additional infections in the vaccine and toxic ingredients as well as any other infections they may have
5) Isolating or restricting close physical contact after a vaccine - the MMR vaccine is a LIVE virus vaccine, and it sheds in body fluids to infect others for 4-6 weeks afterwards. Hence telling your friends and family to get the MMR (or other) vaccines before seeing your newborn baby is pointless or even dangerous, as those that get the vaccine are more likely to actually infect your baby. Similarly, children who have had MMR are potentially infectious for 4-6 weeks afterwards, and should be kept at home and away from siblings, schools, kindergarten and daycare for this same reason
6) Support the immune system and liver detoxification pathways - this can help the child get over the vaccination and any adverse events quicker. This can be done with specific nutritional and/or herbal supplements, good nutrition, quality sleep, some exercise (but not when ill), and good sun exposure (to make vitamin D, which is a huge immune system booster and natural anti-inflammatory hormone).
Conclusion and summary
Health authorities in Australia and overseas are creating a vicious cycle of recommending, and even MANDATING, or forcing people to be vaccinated against measles, which is a LIVE virus vaccine that is known to cause measles in those who receive it, and shed LIVE measles virus in body fluids to infect family members, friends, classmates, and strangers around them, who then get the infection and spread it to others! Even with our constitutional laws of informed consent and no coercion of medical treatments being broken to force parents to vaccinate their children or face financial penalties, and having a 95% vaccine coverage (aka "herd immunity"), IT's NOT WORKING to reduce or stop such infections!
Despite living in a developed country, I see many cases of malnutrition and nutrient deficiencies which are contributing to peoples' health issues. This, together with our stressful and unhealthy lifestyles, a waning short-term immunity from measles vaccines, measles virus shedding from the live vaccines, and scare campaigns from a misinformed media and health departments are causing the alleged increase in measles incidences of late.
The recent increase in incidences of measles is the result of the MMR vaccines failing to cause a lifelong immunity, and not as a result of the failure of some people to vaccinate!
None of the measles vaccines have ever been adequately tested, as they have never used an inert placebo in the control group. This is a deliberate attempt to manipulate the results of safety and efficacy in favour of the vaccine and the manufacturer. As a result, many children suffer lifelong complications of the vaccine which are far worse than the actual measles infection, and many more children die from the measles vaccines than the measles infection.
The government's measles vaccination program is NOT working - it is actually causing far more infections, far more adverse health reactions and deaths from the measles vaccine, compared to the infection that the vaccine is supposed to prevent.
Measles is generally a very mild or benign infection in almost everyone, especially in developed countries which have had next to no deaths from this infection in many years. But the media and medical authorities are making it out to be a huge health issue,with "outbreak" notices daily when even ONE person is suspected of having this infection. As the studies show, support your immune system, have a good dietary intake of all essential nutrients, and use good hygiene practices and your risk will be very small.
Luckily, there are other simpler, and safer natural ways to prevent and treat measles, without buying into the government and media hype which is actually causing more infections and unnecessary concerns.
Do your own due diligence, as it's your health and your family's health after all. Look after your health and that of your family with good preventative strategies as mentioned above, and with any infection, support your immune system to do its job to get rid of the infection, and you will be fine!
You are welcome to share this article in full, or the attached PDF file to share.
| measles_article_2019.pdf |
 RSS Feed
RSS Feed