
For over 7 years I have been warning people on the health dangers and toxicity of sunscreens. I have investigated and written on the ingredients in sunscreens and how they actually INCREASE the risks of skin cancers and melanoma (the most dangerous type) and other health issues.
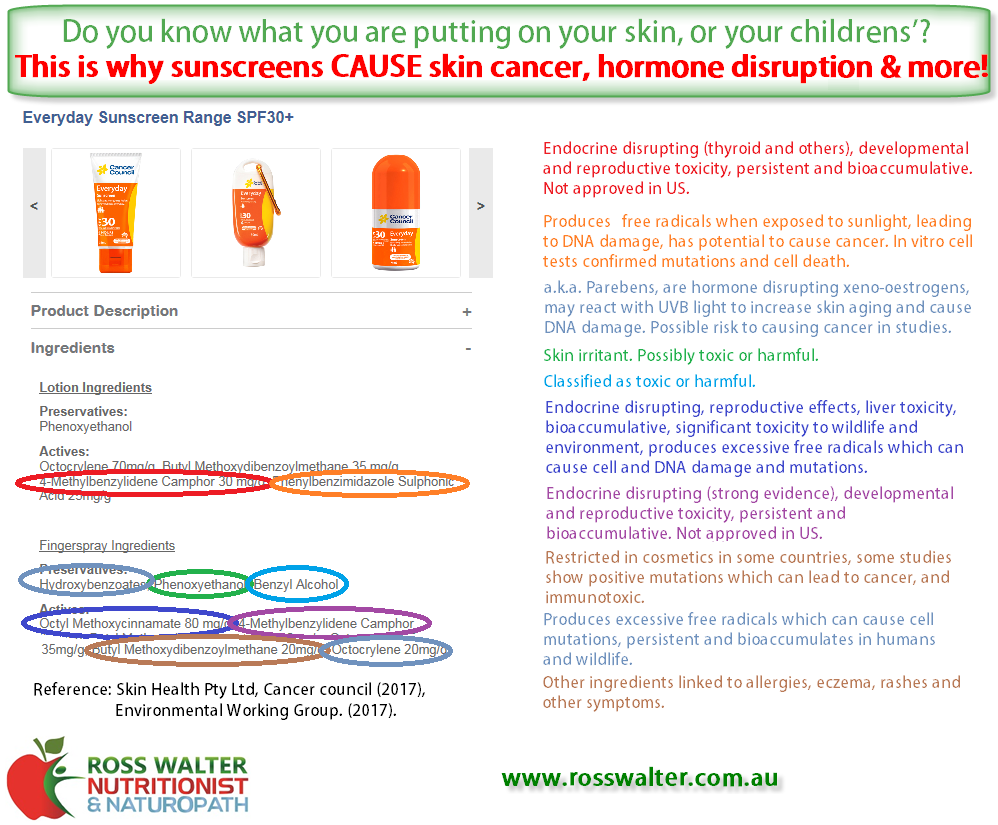
Sunscreens cause more skin cancers (and other cancers) because of their toxic ingredients which are known to cause cancer, but also due to HOW they work - sunscreens block UV-B light to prevent the skin redness and burning, and prevents production of vitamin D which protects against cancer (!), but this gives you a false sense of security to stay outside in the sun longer to be exposed to more UV-A light, which is the one that causes skin damage and skin cancers...
I personally approached sunscreen manufacturers such as the "Cancer Council" about the ingredients they use in their sunscreens, and the many toxic chemicals, hormone disrupting chemicals (affecting male/female hormones or thyroid function), and known cancer-causing chemicals they use. They denied there was any problem, despite many published studies on the chemicals they use causing these health effects.
So every Spring and Summer I call them out on this, so that people are aware and don't use their dangerous sunscreens. There are much better and safer options available.
Karma might have caught up with the "Cancer Council" in May 2022, when their sunscreens had elevated levels of a cancer-causing chemical (Benzene) in them, and they were forced to make this information public and recall some of their products (TGA, 2022). But they have had these dangerous chemicals in their sunscreens for many years and they did nothing. For example, their "everyday" sunscreens had several known cancer-causing chemicals, AND several hormone-disrupting chemicals, and other toxic chemicals, and some chemicals banned in other countries, in ONE product.
Perhaps as a result of this finding, and perhaps my warnings (I'd like to think so!) the Cancer Council changed the ingredients in some of their products recently in 2022. So I checked out their products and ingredients again, and here it is...
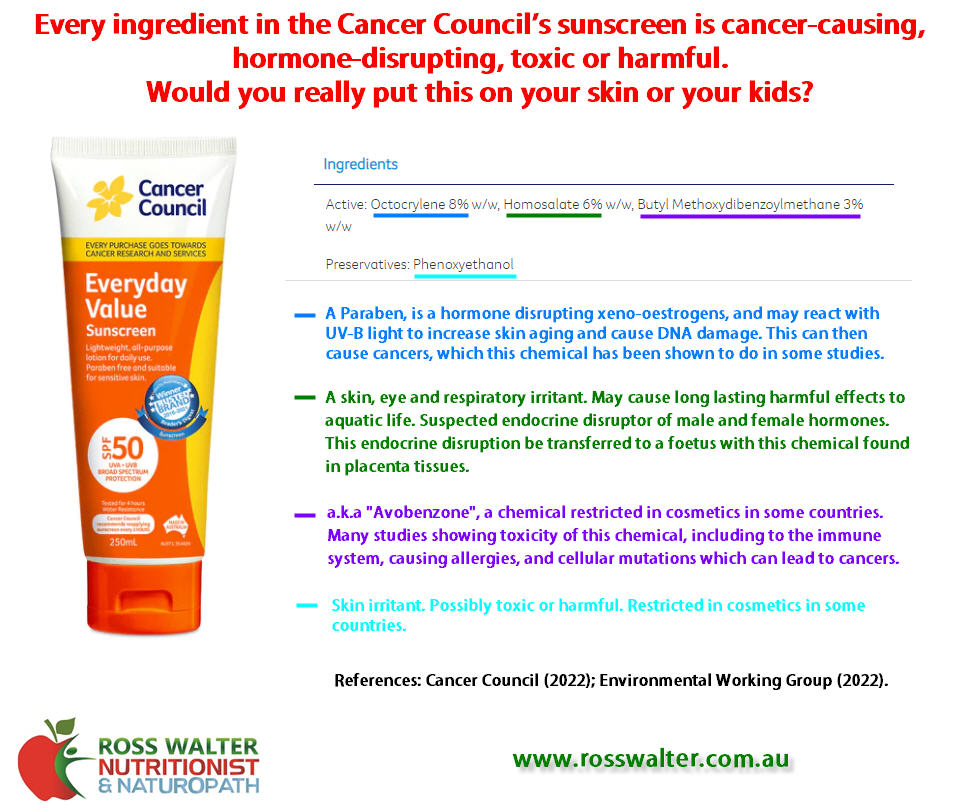
The Cancer Council have so many more products now, mostly with the same toxic ingredients in each product, but some variations too. Their "everyday" sunscreen has one less chemical now, which wasn't one that was known to cause cancer, but did cause neurotoxicity and disruptions to hormones. The "everyday" product still contains 2 cancer-causing chemicals, 2 hormone-disrupting chemicals, and one being damaging the environment or wildlife.
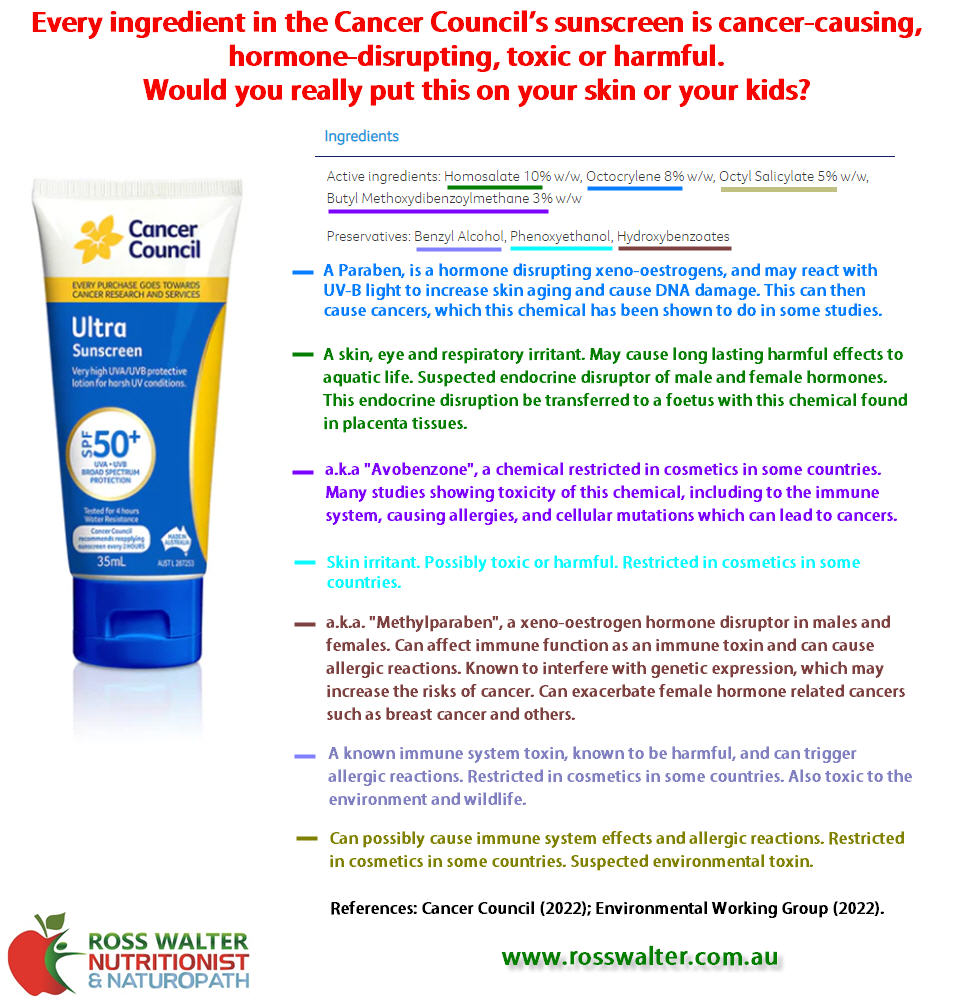
I investigated some of their other sunscreens too, including their "ultra" and "kids" products. The "ultra" product has many more chemicals than the "everyday" product, and more toxic too, with 3 cancer-causing chemicals, 3 hormone-disrupting chemicals, and 3 which are toxic to the environment and wildlife.
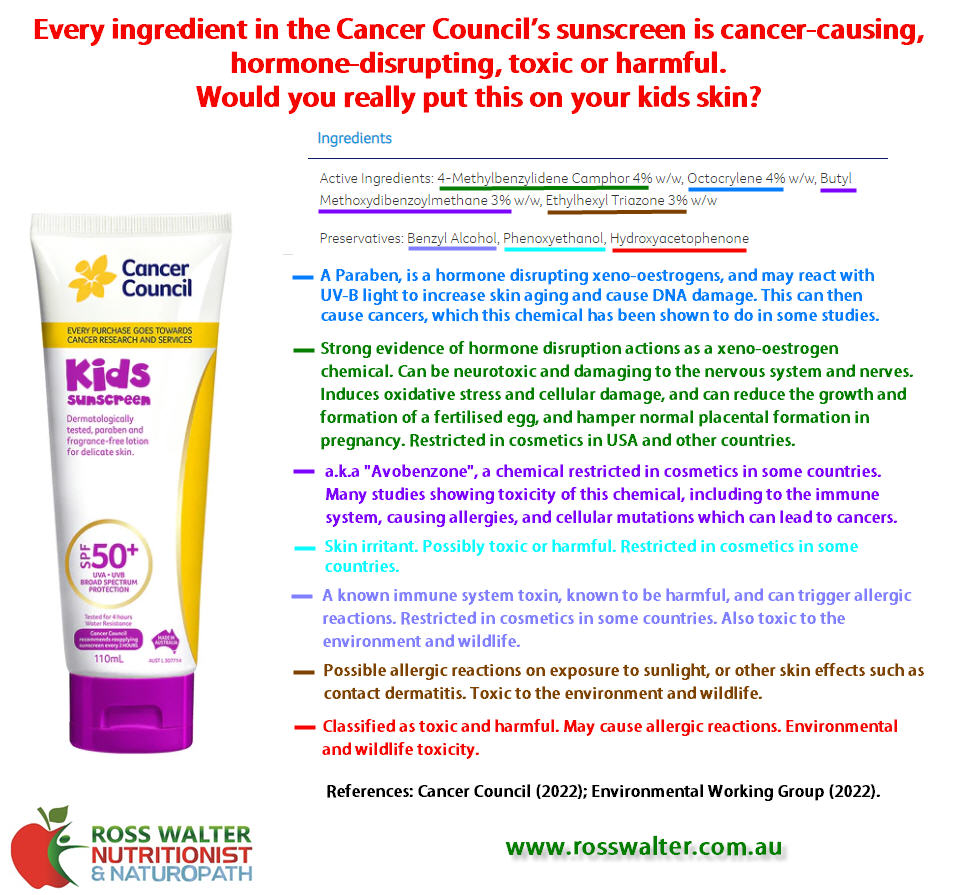
The Cancer Council's "kids" product has the same number of chemicals as the "ultra" product, with most being the same, and containing 2 cancer-causing chemicals, 2 hormone-disrupting chemicals, but 3 which are toxic to the environment or wildlife. If you had children, would you really put this on them now?
The Cancer Council is well named isn't it... adding cancer-causing chemicals to their products which are supposed to prevent cancer, but actually causing it instead.
This article shows the importance of always checking the ingredients and chemicals not just in your foods, but what you put on your skin. What you put on your skin is typically absorbed into your body.
Luckily there are better and safer ways to prevent skin cancers, without the avoidance of healthy sun exposure that you need for vitamin D and other health benefits, and without being exposed to toxic and harmful chemicals.
Stay healthy!
References:
Cancer Council. (2022). Sunscreens. Retrieved 19th November 2022 from https://www.cancercouncilshop.org.au/collections/sunscreen
Therapeutic Goods Administration (TGA). (2022). Multiple Sunscreens Recall - Low levels of benzene detected. Retrieved 20th November 2022 from https://www.tga.gov.au/alert/multiple-sunscreens-recall-low-levels-benzene-detected
Sunscreens cause more skin cancers (and other cancers) because of their toxic ingredients which are known to cause cancer, but also due to HOW they work - sunscreens block UV-B light to prevent the skin redness and burning, and prevents production of vitamin D which protects against cancer (!), but this gives you a false sense of security to stay outside in the sun longer to be exposed to more UV-A light, which is the one that causes skin damage and skin cancers...
I personally approached sunscreen manufacturers such as the "Cancer Council" about the ingredients they use in their sunscreens, and the many toxic chemicals, hormone disrupting chemicals (affecting male/female hormones or thyroid function), and known cancer-causing chemicals they use. They denied there was any problem, despite many published studies on the chemicals they use causing these health effects.
So every Spring and Summer I call them out on this, so that people are aware and don't use their dangerous sunscreens. There are much better and safer options available.
Karma might have caught up with the "Cancer Council" in May 2022, when their sunscreens had elevated levels of a cancer-causing chemical (Benzene) in them, and they were forced to make this information public and recall some of their products (TGA, 2022). But they have had these dangerous chemicals in their sunscreens for many years and they did nothing. For example, their "everyday" sunscreens had several known cancer-causing chemicals, AND several hormone-disrupting chemicals, and other toxic chemicals, and some chemicals banned in other countries, in ONE product.
Perhaps as a result of this finding, and perhaps my warnings (I'd like to think so!) the Cancer Council changed the ingredients in some of their products recently in 2022. So I checked out their products and ingredients again, and here it is...
The Cancer Council have so many more products now, mostly with the same toxic ingredients in each product, but some variations too. Their "everyday" sunscreen has one less chemical now, which wasn't one that was known to cause cancer, but did cause neurotoxicity and disruptions to hormones. The "everyday" product still contains 2 cancer-causing chemicals, 2 hormone-disrupting chemicals, and one being damaging the environment or wildlife.
I investigated some of their other sunscreens too, including their "ultra" and "kids" products. The "ultra" product has many more chemicals than the "everyday" product, and more toxic too, with 3 cancer-causing chemicals, 3 hormone-disrupting chemicals, and 3 which are toxic to the environment and wildlife.
The Cancer Council's "kids" product has the same number of chemicals as the "ultra" product, with most being the same, and containing 2 cancer-causing chemicals, 2 hormone-disrupting chemicals, but 3 which are toxic to the environment or wildlife. If you had children, would you really put this on them now?
The Cancer Council is well named isn't it... adding cancer-causing chemicals to their products which are supposed to prevent cancer, but actually causing it instead.
This article shows the importance of always checking the ingredients and chemicals not just in your foods, but what you put on your skin. What you put on your skin is typically absorbed into your body.
Luckily there are better and safer ways to prevent skin cancers, without the avoidance of healthy sun exposure that you need for vitamin D and other health benefits, and without being exposed to toxic and harmful chemicals.
Stay healthy!
References:
Cancer Council. (2022). Sunscreens. Retrieved 19th November 2022 from https://www.cancercouncilshop.org.au/collections/sunscreen
Therapeutic Goods Administration (TGA). (2022). Multiple Sunscreens Recall - Low levels of benzene detected. Retrieved 20th November 2022 from https://www.tga.gov.au/alert/multiple-sunscreens-recall-low-levels-benzene-detected


 RSS Feed
RSS Feed